

We don’t want you to miss a moment
That’s why EyeMed makes it easy to afford regular eye exams, glasses and contact lenses. Simply enter your zip code, find a plan and enroll online.
Go where you want, get what you want
Access thousands of independent eye doctors, top optical retailers and online providers.


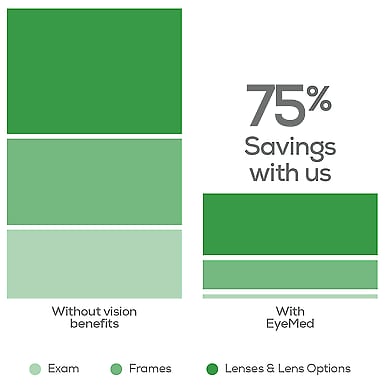
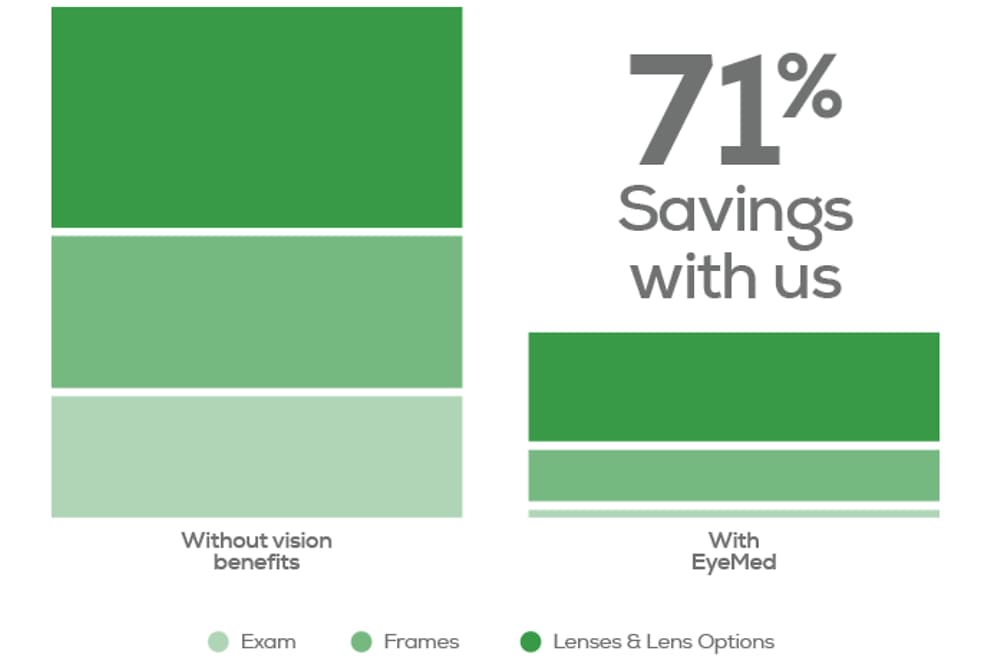
Savings that add up and help keep an eye on your health
EyeMed members save an average of 71% off the retail price of eye exams and glasses at in-network eye doctors2. Even if you see just fine, a regular eye exam can help protect your health.
Got questions?
Is there a waiting period? What’s covered under my plan? How do I submit a claim? Where can I use my benefits? Your top questions answered.
No Benefits will be paid for services or materials connected with or charges arising from: Orthopic or vision training, subnormal vision aids and any associated supplemental testing; Aniseikonic lenses, Medical, pathological, and/or surgical treatment of the eye, eyes or supporting structures; Any Vision Materials (Healthy Plan only); Any Vision Examination, or any corrective eyewear required as a condition of employment; Safety eyewear; Services provided as a result of any workers’ compensation law, or similar legislation, or required by any governmental agency or program whether federal, state or subdivisions thereof; Plano (non-prescription) lenses; Non-prescription sunglasses; or Two pair of glasses in lieu of bifocals (Bold & Bright Plans only). Any sales tax charged by the Provider as part of the transaction for covered services are not covered under this Policy. Fees charged by a Provider for services other than those covered under the Policy must be paid in full by the insured person to the Provider. Such fees or materials are not covered under this policy. Out-of-Network Provider expenses do not apply toward In-Network Provider expenses and In-Network Provider expenses do not apply toward Out-of-network Provider expenses. All providers are not required to carry all brands at all levels. Not available in all states. Some provisions, benefits, exclusions or limitations may vary by state.
Underwritten by Fidelity Security Life Insurance Company® and Fidelity Security Life Insurance Company® of New York, and administered by First American Administrators and InsuranceTPA.com and serviced by EyeMed. Policy numbers VC-133/VCN-12; form numbers M-9157/M-9159/MN-17/MN-19. Policy for Covered California marketplace only: Policy number VC-134; form number M-9172CA/M-9174CA. All frame brands not available at all locations. Discounts are not insured benefits and are subject to change at any time. ADV-VC133-01012016
* - In most states
- 76% savings versus retail — Based on weighted average of sample transactions, EyeMed Book of Business, 2025; EyeMed Insight network/$10 exam copay/$10 materials copay/$150 frame or contact lens allowance. Actual savings will depend on benefits, as well as provider, frame and lens selections. Retail cost based on industry averages, 2025.